Research Article - Central European Journal of Experimental Biology ( 2017) Volume 5, Issue 2
Malignant hyperthermia, FKBP1A, DNA sequencing, Anaesthetics
Malignant Hyperthermia (MH) is a pharmacogenetic syndrome of skeletal muscle, occurs due to abnormal calcium release in the sarcoplasmic reticulum in the skeletal muscles [1]. MH is diagnosed in the laboratory by the in vitro contracture test (IVCT) according to the European Malignant Hyperthermia Group (EMHG). The IVCT test is the only method used for the diagnosis of MH and there is no simple and non-invasive test for MH diagnosis [2].
Mutations in the ryanodine RyR1 channel (RYR1) and Dihydropyridine receptor channel (DHPR) were detected in 70% of the MHS cases. However, DNA sequencing of RYR1 and DHPR (CACNA1S) genes have indicated that about 30% of UK MHS families, have no causative mutations in these two genes [3].
The aim of the present study is to investigate the relationships between MH susceptibility and genes encoding skeletal muscle Ca2+ channels and their accessory proteins. FKBP1A was selected as a candidate gene for DNA sequencing and mutations detection in individuals with no RYR1 or CACNA1S mutations.
FKBP12 are immunophilins encoded by FKBP1A gene and were named due to binding to the immunosuppressant drugs FK506 and rapamycin and their molecular mass (12 kDa). FK506 drugs cause FKBP12 dissociation from RyR1, causing disruption of E-C coupling mechanism. There are two isoforms of FKBP proteins: FKBP12 is expressed in skeletal muscle and interacts with RyR1 [4] and FKBP12.6 is expressed in cardiac muscle where it binds RyR2 [5]. They are also known as (calcium channel stabilizing binding protein) calstabin 1 and 2, respectively. The FKBP12 binding site to RyR1 was located between amino acids 2458 and 2468 of the channel where a mutation was identified in this region that disrupts this FKBP12-RyR1 binding [6]. However, RyR2 interacts with FKBP12.6 and the region between residues 305 and 1937 in the NH2-terminal sequences is essential for RyR2-FKBP12.6 binding [7].
FKBP12 modulates the activity of RyR1 and stabilizes the homotetrameric structure and the closed conformation of the channel [8]. In addition, RyR1 channels demonstrate a longer mean open time and greater open probability when FKBP12 was removed by segregation through binding by its ligands FK506 and rapamycin, suggesting the critical protein-protein interaction [9]. Furthermore, the interaction between the RyR1 channel and the DHPR is reduced by FKBP12 depletion and inhibited by FK506 drugs suggesting that binding of FKBP12 to RyR1 modulates the DHPRRyR1 interaction [10]. In addition, dissociation of RyR-FKBP12 interaction results in increased sensitivity of RyR1 to halothane, thus dysregulation of Ca2+ release by RyR1 channel leads to muscle contracture. This alteration in the FKBP12 binding to RyR1 was proposed to cause MH susceptibility [11].
In this study, DNA sequencing was carried out to elucidate the genetic variants in the 30% of MHS families with no RYR1 or CACNA1S mutations. FKBP1A was selected as a candidate gene for DNA sequencing due to its regulation of RyR1 [12] and mediation of intracellular calcium release in skeletal and cardiac muscle [6]. In addition, an FKBP12- deficient mouse model showed significantly abnormal excitation-contraction coupling and altered intracellular Ca2+ release [13]. The FKBP1A coding sequence is reasonably short and represented by only five exons, making it a good potential candidate for DNA sequencing.
Genomic DNA was extracted from blood samples obtained from 50 UK Malignant Hyperthermia Susceptible patients who were positive for IVCT and negative for all causative mutations in RYR1 and DHPR (CACNA1S) genes according to the European Malignant Hyperthermia Group. 200 DNA samples of human random control were used as the control. These DNA samples were obtained from UK Caucasian blood donors (Sigma-Aldrich). The control samples were recommended to use as Reference Standards for routine quality controls in the laboratory.
DNA was extracted from whole blood samples in EDTA. DNA concentration was quantified using a NanoDrop ND- 1000 spectrophotometer (Thermo Scientific, Wilmington, USA) by measuring the absorbance at 260 and 280 nm. Tris-EDTA (TE) buffer was used as a blank sample for all genomic DNA measurements. DNA purity was determined by the A260/A280 ratio.
A genomic structure of FKBP1A was identified using National Centre for Biotechnology Information (NCBI) and Ensembl databases. Exon-specific oligonucleotide primers were designed using software (Primer 3) obtained online at http://frodo.wi.mit.edu [14]. The designed primers were blasted in the Ensembl database to confirm specificity of each. The primers were selected to cover the entire coding sequence (exons) and 10-20 bp of the flanking sequence of each exon to include the splice site sequence.
Genomic DNA of the entire coding sequence of FKBP1A was amplified by PCR in a 20 μl PCR reaction mixture. PCR reactions containing ddH2O instead of DNA were used with each PCR experiment as negative control. PCR was carried out using Thermo Prime Taq DNA polymerase according to the manufacturer’s recommended protocol. The PCR reactions were optimised to produce a PCR product without non-specific bands. Each 20 μl PCR reaction comprised 1x PCR buffer, 0.2 mM of dNTPs, 1.5 mM of MgCl2, 20 pmol of each primer, 0.025 U of ThermoPrime DNA polymerase and 10 ng genomic DNA from MHS patients. The amplification process was carried out using 2700 PCR Thermocycler (Applied Biosystems) and consisted of a 5 min denaturation step at 94°C followed by 30 cycles of 94°C for 45 s, an annealing step for the primer at 59-61°C for 45 s, an extension step at 72°C for 45 s and a final extension step at 72 ºC for 7 min.
Primers were designed to amplify the entire coding sequence of FKBP1A. Five pairs of primers were utilized to amplify exons 1 and 2 in combination, exon 3 and 4 and two different pair of primers as two fragments amplified exon 5. The optimum MgCl2 concentration was 1.5 mM and optimum annealing temperature was 60°C for all pairs of primers (Table 1).
| Exon | Primer Sequence (5' to 3') | Products Size (bp) |
|---|---|---|
| 1 & 2 | F: GGAGGTCTCGGGGCTTCT R: ACAGCCGCCGATTCAGAC |
572 |
| 3 | F: CATGTTACAGTCGTCTTTTTCACA R: AAACAAAACAAATGAGAGAGCAT |
163 |
| 4 5A | F: TCTGTCTTCCTTGTTCTTTTCACA R: GCCCTTCAGTATTCCATTTC F: CACAGATTTTCTGTCCCCAAC R: CAAAGGCTCTCCCCATCC |
215 573 |
| 5B | F: AAAAGCCCTACCTAAAACTGAGG R: GGGGAGGCACCTGAAAATA |
628 |
Table 1: Primers and PCR optimisation to amplify FKBP1A sequence The PCR reaction utilized 1.5 mM of MgCl2 for all primers PCR amplification
DNA direct sequencing was performed using Sanger chain termination technique [15]. The sequencing was carried out using the BigDye terminator sequencing kit according to the manufacturer’s instructions (ABI 3100 Genetic Analyser, Applied Biosystems). PCR products that prepared for DNA sequencing, were purified from dNTPs and unincorporated primers using the enzymatic method (ExoSAP-IT®).
Sequencing data analysis
Sequencing chromatograms were analysed using Sequencing Analysis Software v5.3® Software v2.6 (Applied BioSystems). The sequencing data were aligned to the reference sequence of each DNA in the Ensemble database to detect any novel genetic variant. As the primers were designed to include 10-20 bp of the flanking regions of each targeted DNA sequence the sequencing chromatograms were also analysed in the region of the 20 bases flanking the target DNA sequence. The data were considered as valid and accepted when the chromatograms have obvious peaks for conclusive results. If any variations were detected, the DNA sample was double checked in reverse and forward sequence.
Herewith the reference sequence of mRNA for FKBP1A gene:
TTTCCGGGACGTCGCGCGCCGTGTGGGGCGCGCACGCAGGGCTGGGCGTGAGGGGGCGTGCGC GTGCGCAGGCGACGCGCCGAGGTACTAGGCAGAGCCGTGGAACCGCCGCCAGGTCGCTGTTGG TCCACGCCGCCCGTCGCGCCGCCCGCCCGCTCAGCGTCCGCCGCCGCCATGGGAGTGCAGGTGGAAACCATCTCCCCAGGAGACGGGCGCACCTTCCCCAAGCGCGGCCAGACCTGCGTGGTGCA CTACACCGGGATGCTTGAAGATGGAAAGAAATTTGATTCCTCCCGGGACAGAAACAAGCCCTTTAAGTTTATGCTAGGCAAGCAGGAGGTGATCCGAGGCTGGGAAGAAGGGGTTGCCCAGATGA GTGTGGGTCAGAGAGCCAAACTGACTATATCTCCAGATTATGCCTATGGTGCCACTGGGCACCCAGGCATCATCCCACCACATGCCACTCTCGTCTTCGATGTGGAGCTTCTAAAACTGGAATGA CAGGAATGGCCTCCTCCCTTAGCTCCCTGTTCTTGGATCTGCCATGGAGGGATCTGGTGCCTCCAGACATGTGCACATGAATCCATATGGAGCTTTTCCTGATGTTCCACTCCACTTTGTATAGA CATCTGCCCTGACTGAATGTGTTCTGTCACTCAGCTTTGCTTCCGACACCTCTGTTTCCTCTTCCCCTTTCTCCTCGTATGTGTGTTTACCTAAACTATATGCCATAAACCTCAAGTTATTCATT TTATTTTGTTTTCATTTTGGGGTGAAGATTCAGTTTCAGTCTTTTGGATATAGGTTTCCAATTAAGTACATGGTCAAGTATTAACAGCACAAGTGGTAGGTTAACATTAGAATAGGAATTGGTGT TGGGGGGGGGGTTTGCAAGAATATTTTATTTTAATTTTTTGGATGAAATTTTTATCTATTATATATTAAACATTCTTGCTGCTGCGCTGCAAAGCCATAGCAGATTTGAGGCGCTGTTGAGGACT GAATTACTCTCCAAGTTGAGAGATGTCTTTGGGTTAAATTAAAAGCCCTACCTAAAACT GAGGTGGGGATGGGGAGAGCCTTTGCCTCCACCATTCCCACCCACCCTCCCCTTAAACCCTCTGCCTTTGAAAGTAGATCATGTTCACTGCAATGCTGGACACTACAGGTATCTGTCCCTGGGCC AGCAGGGACCTCTGAAGCCTTCTTTGTGGCCTTTTTTTTTTTTCATCCTGTGGTTTTTCTAATGGACTTTCAGGAATTTTGTAATCTCATAACTTTCCAAGCTCCACCACTTCCTAAATCTTAAGA ACTTTAATTGACAGTTTCAATTGAAGGTGCTGTTTGTAGACTTAACACCCAGTGAAAGCCCAGCCATCATGACAAATCCTTGAATGTTCTCTTAAGAAAATGATGCTGGTCATCGCAGCTTCAG CATCTCCTGTTTTTTGATGCTTGGCTCCCTCTGCTGATCTCAGTTTCCTGGCTTTTCCTCCCTCA GCCCCTTCTCACCCCTTTGCTGTCCTGTGTAGTGATTTGGTGAGAAATCGTTGCTGCACCCTTCCCCCAGCACCATTTATGAGTCTCAAGTTTTATTATTGCAATAAAAGTGCTTTATGCCGGCT TTTCTCAGAAAAAAAAAA
In the current study, DNA sequencing for the entire coding DNA sequence of FKBP1A represented by the six exons and flanking sequences was performed successfully. Screening of the FKBP1A coding sequence for MH potential causative mutations was performed in 50 MHS individuals in Figure 1. Nevertheless, no causative mutations or any novel genetic variants were detected in the 50 sequences in comparison to the reference genome [15].
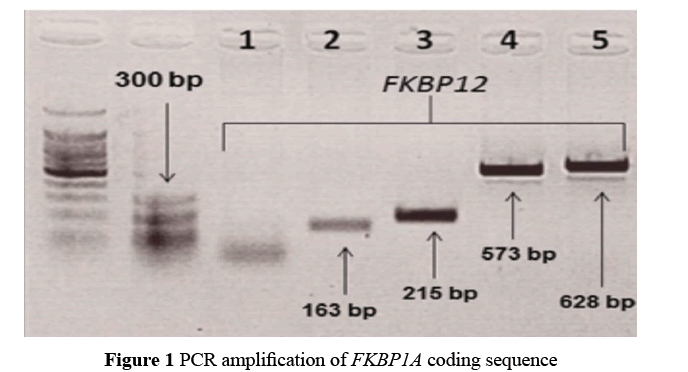
Figure 1: PCR amplification of FKBP1A coding sequence
Agarose gel electrophoresis of PCR products for the encoding sequence of FKBP1A. Lanes 1 and 2 represent faint PCR products utilizing primers to amplify exon 1 and 2 together then exon 3 of FKBP1A, respectively. These two primers need more optimisation as shown in Figure 2. Lane 3 represents amplification of exon 4. Lanes 4 and 5 indicate detection of exon 5 in two fragments. The amplification was performed using 60°C annealing temperatures and 1.5 mM of MgCl2 [16].
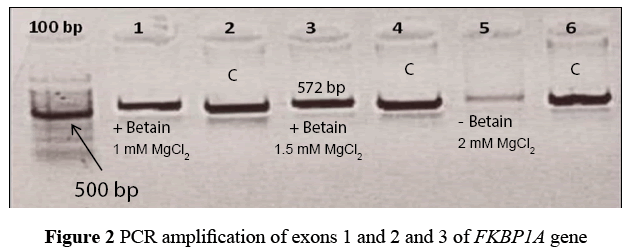
Figure 2: PCR amplification of exons 1 and 2 and 3 of FKBP1A gene
Agarose gel electrophoresis of repeated PCR amplification of exons 1 and 2 of FKBP1A gene with different PCR conditions. Exon 1 and 2 were amplified successfully together using one pair of primers. The different PCR conditions used include different annealing temperatures and different concentrations of MgCl2 mM. Lanes 1 and 3 represent FKBP1A amplification utilising betaine in the reaction with different annealing temperatures and concentration of MgCl2 mM while in lane 5, betaine was not used. Lanes 2, 4 and 6 represent amplification of control DNA sequence.
Agarose gel electrophoresis shows amplification of exon 3 of the FKBP1A gene. Lanes 1 and 2 represent FKBP1A exon 3 amplification utilising a similar annealing temperature as shown in Figure 3, lane 1 without betaine and lane 2 with betaine. Lanes 3 and 4 are used as control where two different annealing temperatures were used to amplify exon 4, in lane 3 without betaine and in lane 4 with betaine [17].
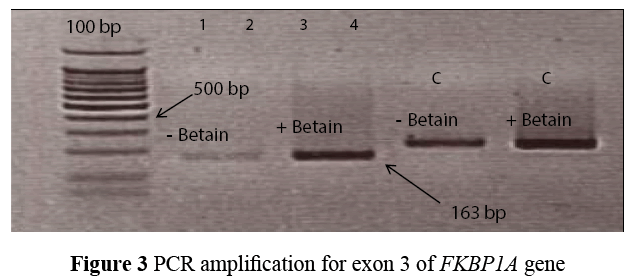
Figure 3: PCR amplification for exon 3 of FKBP1A gene
In our study, DNA sequencing of the FKBP1A coding sequence in 50 MHS individuals revealed no causative mutations or any novel genetic variants were detected in the entire sequence of the gene.
Nowadays, genetic testing of MH susceptibility is the primary goal of MH research to replace the IVCT test with less invasive and convenient diagnostic test. Analysis of previous studies in UK MHS families indicates the involvement of several interacting genes other than RYR1 and has confirmed the genetic heterogeneity of MH [16,17].
In this study, according to the selection criteria, FKBP1A was chosen for DNA sequencing for several important characteristics of FKBP12 protein. These include its expression in skeletal muscle and interaction with RyR1 [4], FKBP12 modulates the activity of RyR1 and stabilizes its structure at the closed conformation of the channel [8]. In addition, FKBP1A was proposed as an MH candidate gene [11]. However, DNA sequencing analysis of the coding sequence of FKBP1A in our study revealed no novel sequence variants or MH causal mutations. One of the limitations of this study is the small number of the study sample (50 MHS DNA). However, this number of DNA samples is acceptable as MH is considered as rare genetic syndrome. Further studies for screening of MH mutations in FKBP1A gene in different populations or screening of MH mutations in different genes are suggested.
In our study, DNA sequencing indicated no any novel mutations in FKBP1A gene. These findings exclude FKBP1A as candidate gene for MH susceptibility at least in a UK MH population. Therefore, DNA sequencing of other potential candidate genes, which contribute to the calcium release unit, are suggested for detection of causative mutations associated with MH susceptibility in individuals with no RYR1 or CACNA1S mutations.
This is the first time that sequencing of the FKBP1A gene has been performed in MHS patients who have no RYR1 or CACNA1S mutations. However, the FKBP1A screening project results exclude FKBP1A as likely candidate gene for MH susceptibility.
This work was supported by donations from the British Malignant Hyperthermia Association and a research scholarship from King Fahad Security College, Saudi Arabia.